I have been reviewing the ground reaction forces (GRF) analysis and have encountered a few questions that I would greatly appreciate your guidance on. This is only for a gait patient who turns the direction of movement.
Ground Reaction Forces Analysis:
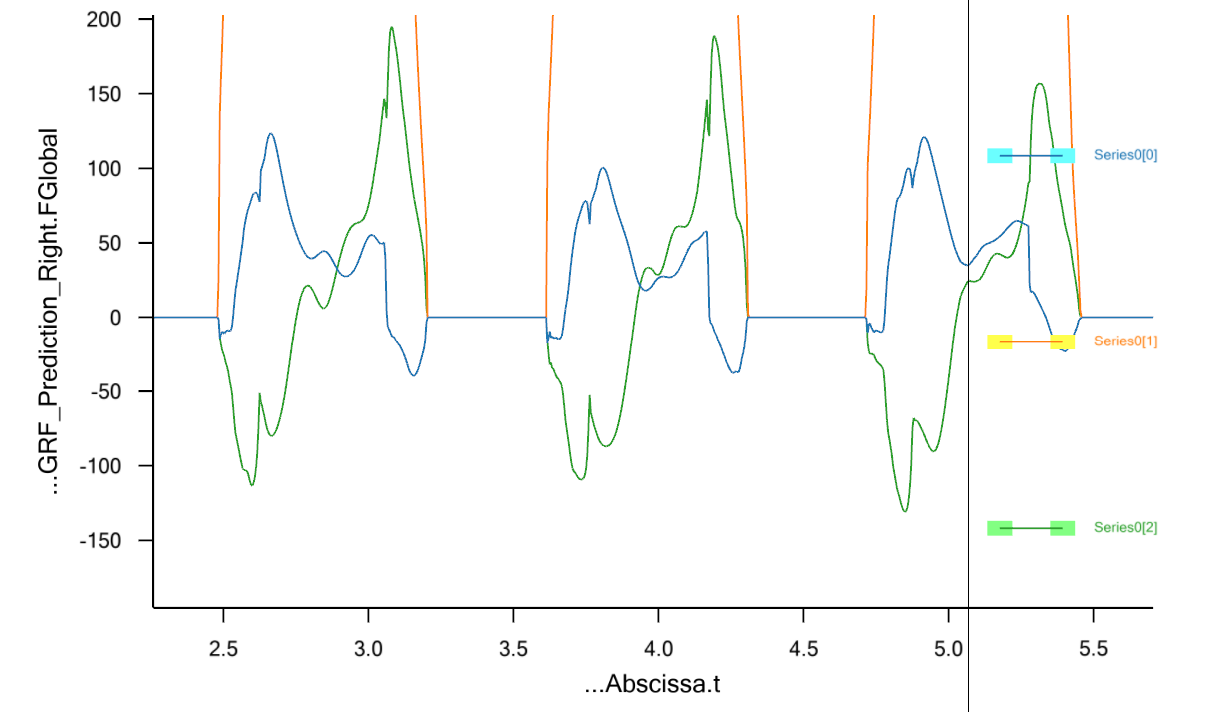
I am analyzing the GRF in the global coordinate system, and the curves seem to align with what is described in the literature. Specifically, the blue curve represents the force in the X-direction (medio-lateral), the orange curve corresponds to the force in the Y-direction (vertical), and the green curve shows the force in the Z-direction (anterior-posterior).
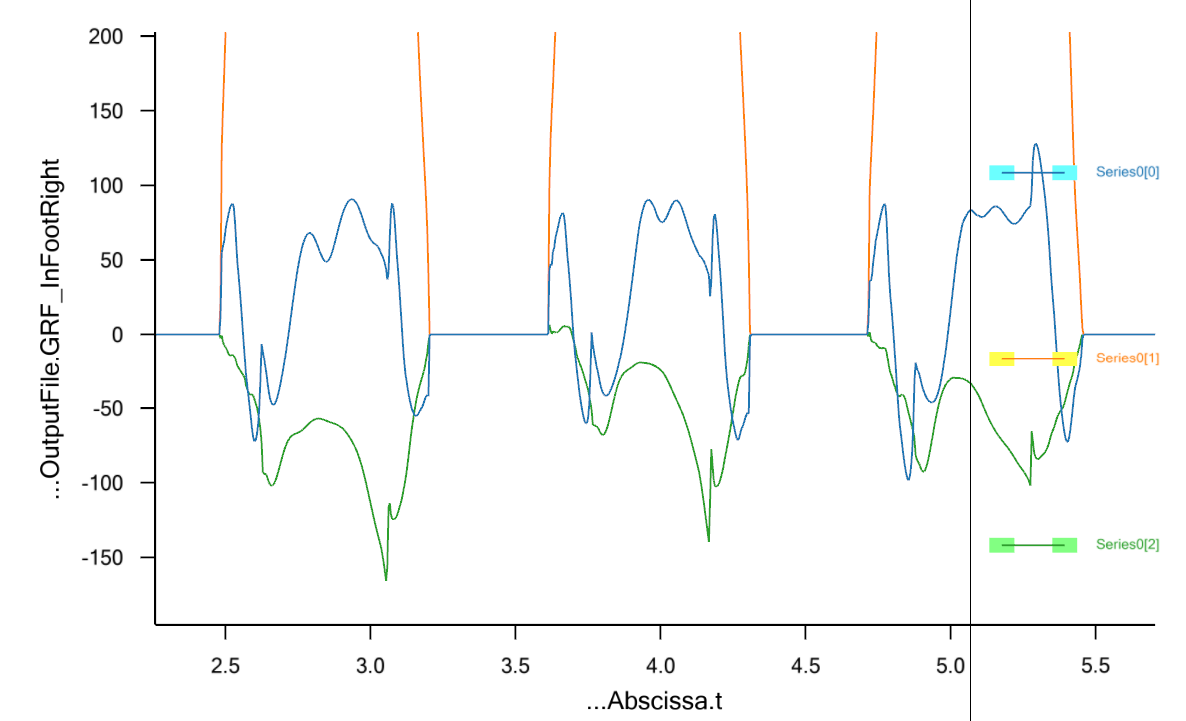
However, as the patient may not always walk in a straight line and could shift to the left or right, I am wondering whether it is necessary to transform the X and Z components into the foot’s local coordinate system? My concern is how to compare the results with the literature, as the graphs appear quite different. Should I use the results in the global coordinate system, or would transforming them to the foot's coordinate system provide a more accurate comparison?
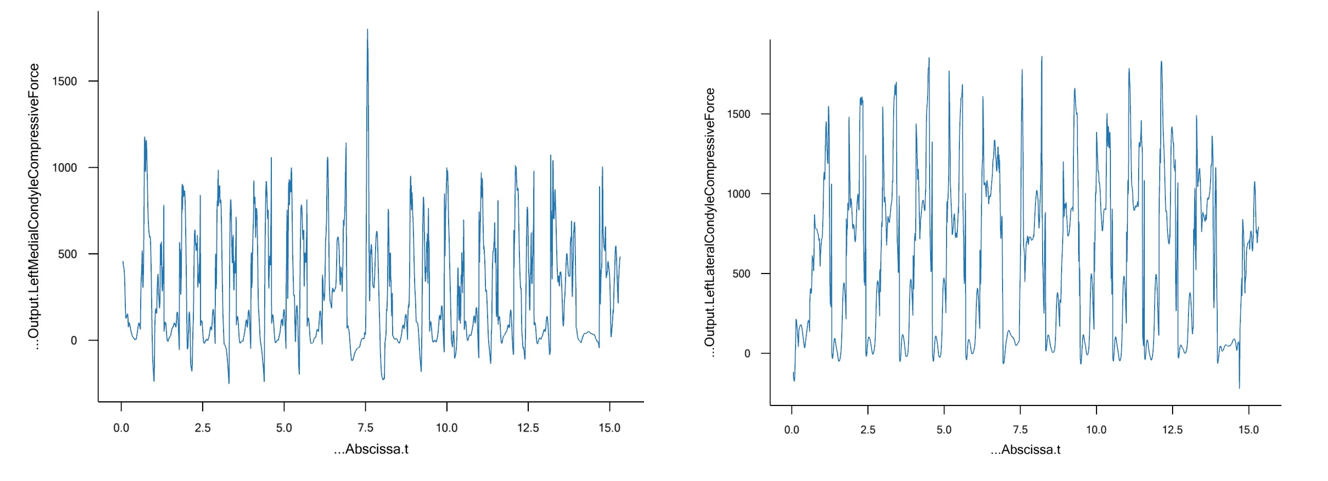
Regarding the knee joint forces, I have separated the components into medial and lateral forces. However, I noticed that the graphs show significant peaks in the data.
You are right, you should consider using GRF in the local system of the foot. I believe that is the best approach to compare anterior-posterior and medio-lateral directions, especially since you mention that the subject turns. Is it the GRF prediction model that you are using here?
Regarding the knee joint force analysis, can you please describe how have you separated the components into medial and lateral forces? Do you see similar spikes when you just look at the knee joint reaction force? Can you please also tell me which version of AMMR are you using?
Thanks for your input! That’s exactly what I saw in this forum—when the patient reverses direction, they suggested that using the local coordinate system would be more appropriate.
Do you think it would be interesting to compare the global and local reference in this context?
Regarding the model I’m using, it’s the BVH_Xsens, as the data was collected using Xsens.
For the knee joint reaction forces in both the right and left knees, I first measure the reaction forces and moments at the knee joint using the AnyForceMomentMeasure function. This allows me to extract the forces and moments from the knee joint constraints in the model. I then transform these values into the tibia’s coordinate system to ensure consistency in the reference frame.
To separate the forces into medial and lateral components, I follow an approach based on this study:(https://doi.org/10.1080/23335432.2018.1499442). I calculate the distance between the medial and lateral epicondyles of the femur, an anatomical measurement that helps determine the moment arms for each condyle. By estimating the width of the femoral condyles and the intercondylar notch, I apply specific multipliers to compute these dimensions. These calculations are performed for both knees, and the moment arms for the medial and lateral condyles are derived accordingly.
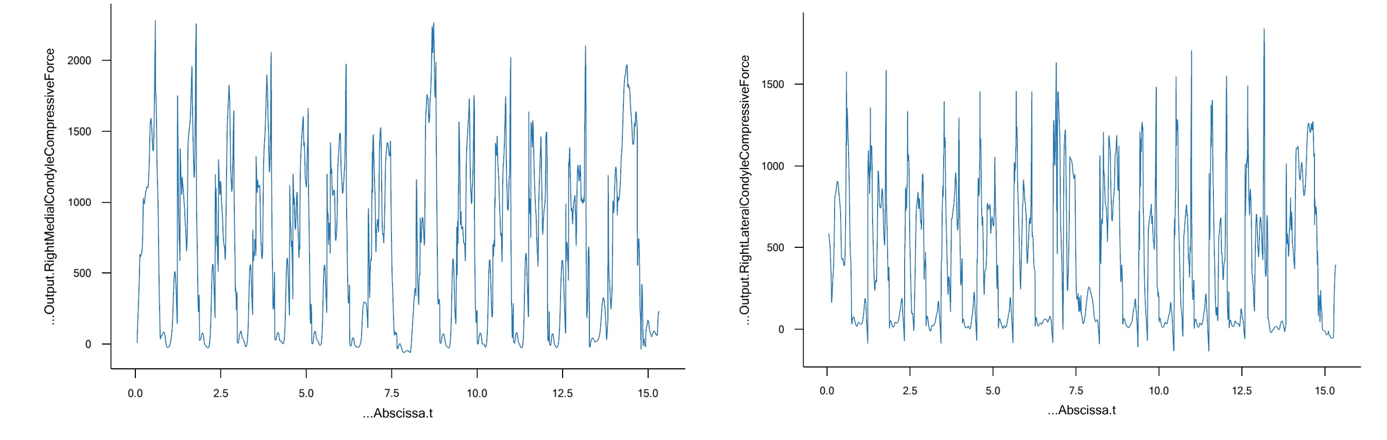
Once the moment arms are established, I compute the compressive forces at the medial and lateral condyles. The medial force is determined using the forces in the shank coordinate system along with the corresponding moment arms. The lateral force is then obtained as the difference between the total force in the tibia coordinate system and the medial force.
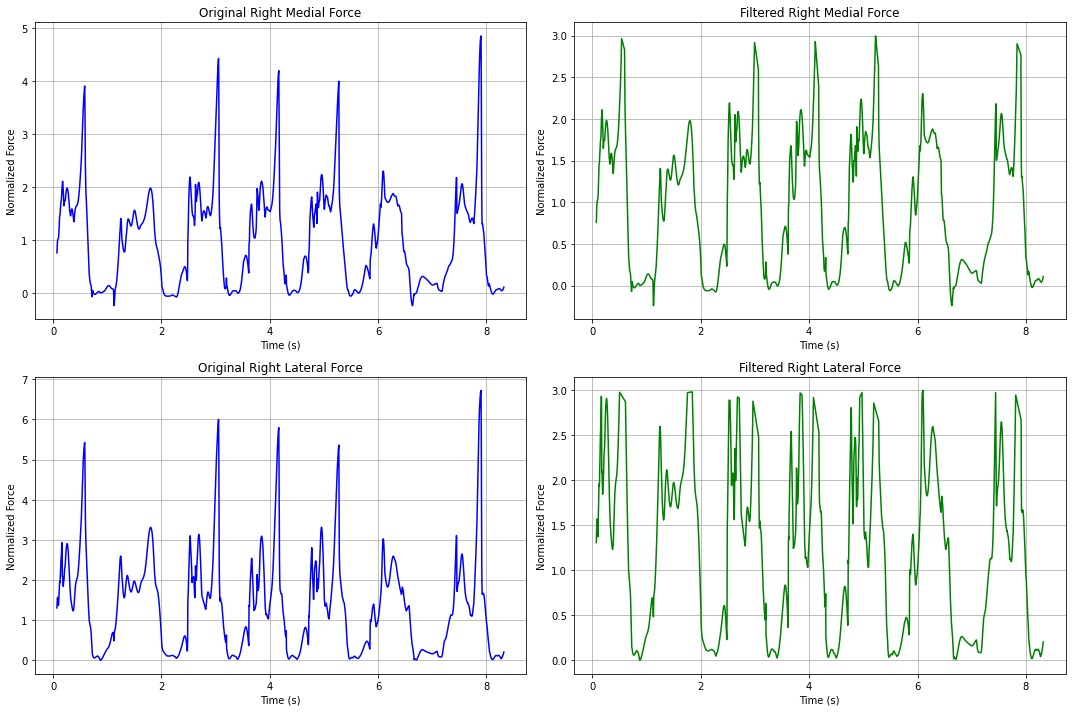
Additionally, when analyzing the knee joint reaction forces, I observe the peaks in these forces:
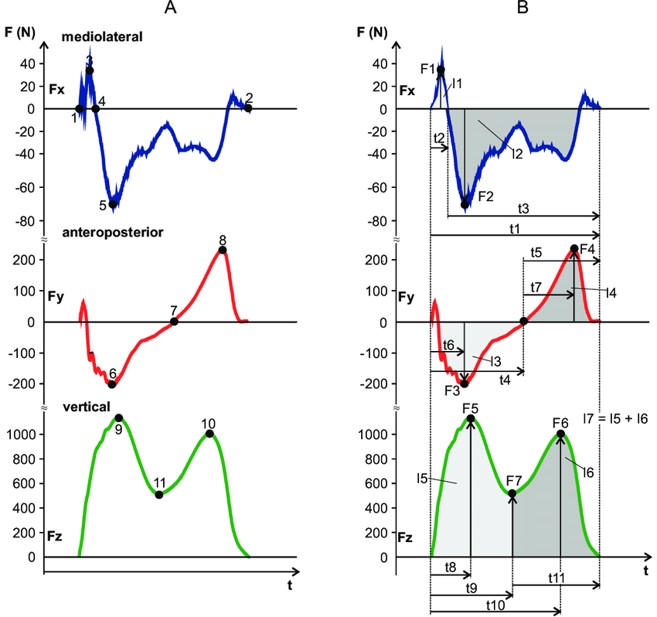
Regarding the ground reaction force (GRF), it is also important to see how it is expressed in literature. You would want to be consistent with the literature approach.
Regarding the joint reaction force, is it possible for you to share the knee Proximo Distal force, since you mentioned compressive force before? Also, can you maybe just zoom in to the first 5 seconds of the trial? It would be easier to understand the graph. Regardless, there are some issues that affect the second peak, that is the peak at toe off, in the knee compressive force. This essentially is due to how the load is shared between gastrocnemius and soleus, which in turn depends on their relative strength. If you are using the simple muscle model, the relative strength is determined from the physical cross section area (PCSA) from the TLEM project. But there is more to it. At toe off, the muscles are close to their range of motion, so the relative difference in the strength is probably not correct. There is also the force-velocity relation that is not taken into account. You could try with the 3 element muscle model, but it also requires that you calibrate the muscles and that is also tricky. Unfortunately, it's not an easy issue to fix. We tried to improve the muscle path of gastrocnemius and soleus in AMMR 3.0 to improve this problem of second peak, but perhaps more can be done.
There is also the possibility that kinematics affects the knee joint reaction. If the GRF vector is too far forward of the knee around toe-off (just heel strike of the other foot), then it can induce the use of gastrocnemius. This can happen in the GRF prediction model because of how the contact conditions are set up. You could try to adjust the contact thresholds slightly for your model. Perhaps, there is some offset for the shoe and so on.
Generally, you should also check if the motion is not noisy. You can see the acceleration of the Centre of Mass, or some other segment, to see if it is too noisy.